
Historical development of bronchoscopy
The broad concept of bronchoscope should include rigid bronchoscope and flexible (flexible) bronchoscope.
1897
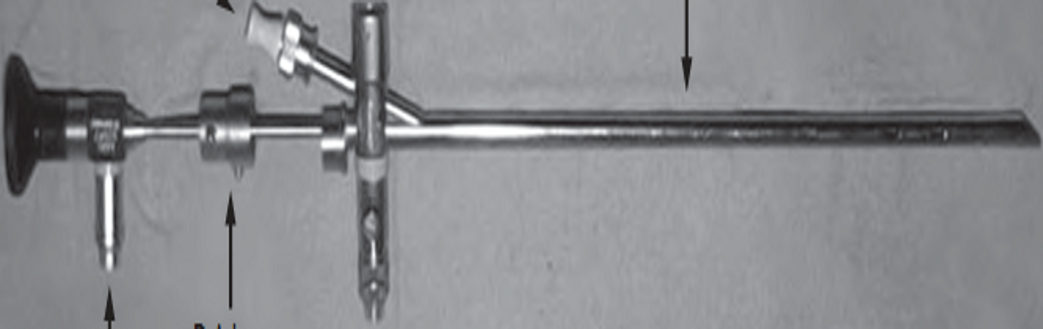
In 1897, German laryngologist Gustav Killian performed the first bronchoscopic surgery in history - he used a rigid metal endoscope to remove a bony foreign body from a patient's trachea.
1904
Chevalier Jackson in the United States manufactures the first bronchoscope.
1962
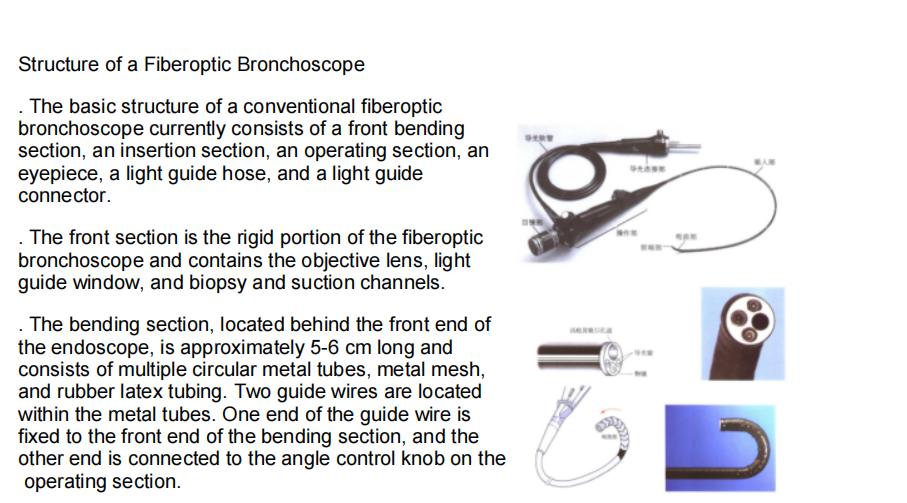
Japanese doctor Shigeto Ikeda developed the first fiberoptic bronchoscope. This flexible, microscopic bronchoscope, measuring just a few millimeters in diameter, transmitted images through tens of thousands of optical fibers, enabling easy insertion into segmental and even subsegmental bronchi. This breakthrough allowed doctors to visually observe structures deep within the lungs for the first time, and patients could tolerate the examination under local anesthesia, eliminating the need for general anesthesia. The advent of the fiberoptic bronchoscope transformed bronchoscopy from a invasive procedure to a minimally invasive examination, facilitating the early diagnosis of diseases such as lung cancer and tuberculosis.
1966
In July 1966, Machida produced the world's first true fiberoptic bronchoscope. In August 1966, Olympus also produced its first fiberoptic bronchoscope. Subsequently, Pentax and Fuji in Japan, and Wolf in Germany, also released their own bronchoscopes.
Fiberoptic bronchoscope:

Olympus XP60, outer diameter 2.8mm, biopsy channel 1.2mm
Compound bronchoscope:

Olympus XP260, outer diameter 2.8mm, biopsy channel 1.2mm
History of pediatric bronchoscopy in China
The clinical use of fiberoptic bronchoscopy in children in my country began in 1985, pioneered by children's hospitals in Beijing, Guangzhou, Tianjin, Shanghai, and Dalian. Building on this foundation, in 1990 (officially established in 1991), Professor Liu Xicheng, under the guidance of Professor Jiang Zaifang, established China's first pediatric bronchoscopy room at Beijing Children's Hospital affiliated with Capital Medical University, marking the official establishment of China's pediatric bronchoscopy technology system. The first fiberoptic bronchoscopy examination in a child was performed by the Respiratory Department at the Children's Hospital affiliated with Zhejiang University School of Medicine in 1999, making it one of the first institutions in China to systematically implement fiberoptic bronchoscopy examinations and treatments in pediatrics.
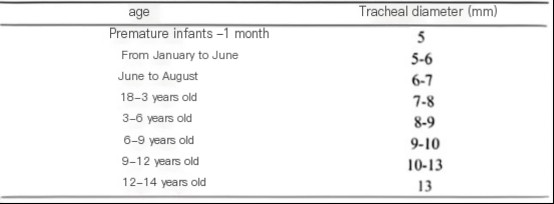
Tracheal diameter of children at different ages
How to choose different models of bronchoscopes?
The choice of pediatric bronchoscope model should be determined based on the patient's age, airway size, and the intended diagnosis and treatment. The "Guidelines for Pediatric Flexible Bronchoscopy in China (2018 Edition)" and related materials are the primary references.
Bronchoscope types primarily include fiberoptic bronchoscopes, electronic bronchoscopes, and combination bronchoscopes. There are many new domestic brands on the market, many of which are of high quality. Our goal is to achieve a thinner body, larger forceps, and clearer images.
Some flexible bronchoscopes are introduced:

Model Selection:
1. Bronchoscopes with a diameter of 2.5-3.0mm:
Suitable for all age groups (including neonates). Currently available on the market are bronchoscopes with outer diameters of 2.5mm, 2.8mm, and 3.0mm, and with a 1.2mm working channel. These bronchoscopes can perform aspiration, oxygenation, lavage, biopsy, brushing (fine-bristle), laser dilatation, and balloon dilatation with a 1mm diameter pre-dilatation section and metal stents.
2. Bronchoscopes with a diameter of 3.5-4.0 mm:
Theoretically, this is suitable for children over one year old. Its 2.0 mm working channel allows for procedures such as electrocoagulation, cryoablation, transbronchial needle aspiration (TBNA), transbronchial lung biopsy (TBLB), balloon dilatation, and stent placement.
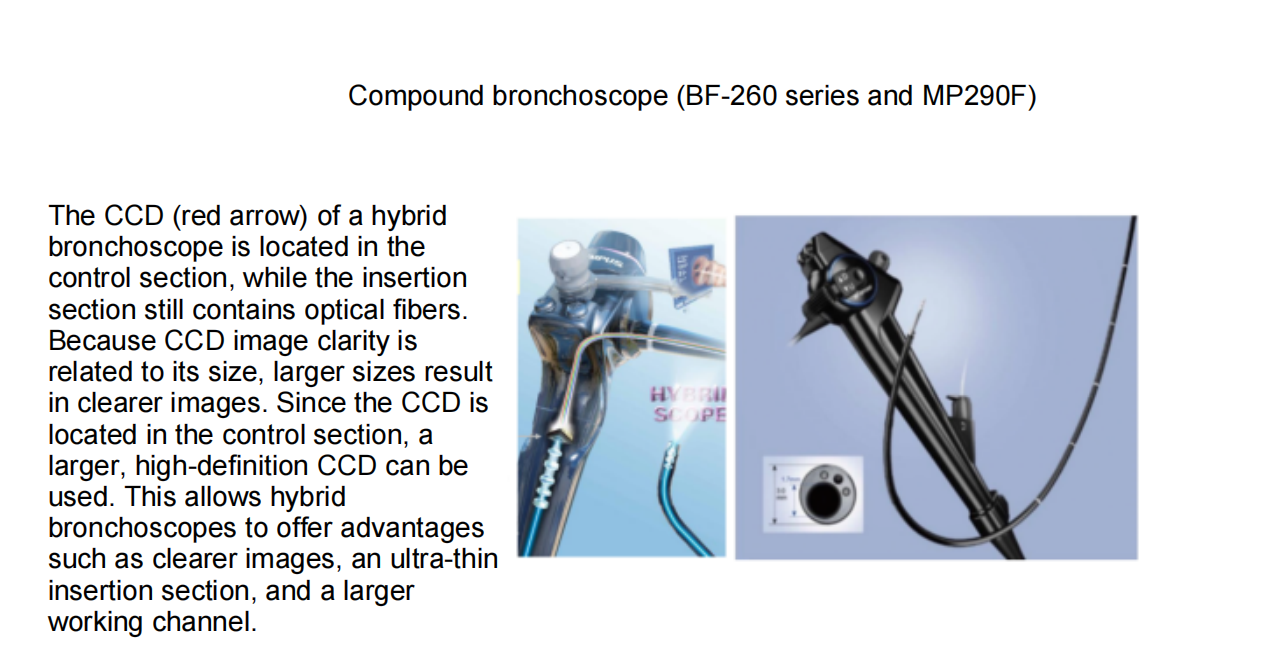
The Olympus BF-MP290F is a bronchoscope with an outer diameter of 3.5 mm and a 1.7 mm channel. Tip outer diameter: 3.0 mm (insertion portion ≈ 3.5 mm); channel inner diameter: 1.7 mm. It allows passage of 1.5 mm biopsy forceps, 1.4 mm ultrasound probes, and 1.0 mm brushes. Note that 2.0 mm diameter biopsy forceps cannot enter this channel. Domestic brands like Shixin also offer similar specifications. Fujifilm's next-generation EB-530P and EB-530S series bronchoscopes feature an ultra-thin scope with an outer diameter of 3.5 mm and a 1.2 mm inner diameter channel. They are suitable for the examination and intervention of peripheral lung lesions in both pediatric and adult settings. They are compatible with 1.0 mm cytology brushes, 1.1 mm biopsy forceps, and 1.2 mm foreign body forceps.
3. Bronchoscopes with a diameter of 4.9 mm or greater:
Generally suitable for children aged 8 years and over weighing 35 kg or more. The 2.0 mm working channel allows for procedures such as electrocoagulation, cryoablation, transbronchial needle aspiration (TBNA), transbronchial lung biopsy (TBLB), balloon dilatation, and stent placement. Some bronchoscopes have a working channel greater than 2 mm, making them more convenient for interventional procedures.
Diameter
4. Special Cases: Ultrathin bronchoscopes with an outer diameter of 2.0 mm or 2.2 mm and no working channel can be used to examine the distal small airways of premature or full-term infants. They are also suitable for airway examinations in young infants with severe airway stenosis.
In short, the appropriate model should be selected based on the patient's age, airway size, and diagnostic and treatment needs to ensure a successful and safe procedure.
Some things to note when choosing a mirror:
Although 4.0mm outer diameter bronchoscopes are suitable for children over 1 year old, in actual operation, 4.0mm outer diameter bronchoscopes are difficult to reach the deep bronchial lumen of children aged 1-2 years old. Therefore, for children under 1 year old, 1-2 years old, and weighing less than 15kg, thin 2.8mm or 3.0mm outer diameter bronchoscopes are generally used for routine operations.
For children aged 3-5 years and weighing 15kg-20kg, you can choose a thin mirror with an outer diameter of 3.0mm or a mirror with an outer diameter of 4.2mm. If imaging shows that there is a large area of atelectasis and sputum plug is likely to be blocked, it is recommended to use a mirror with an outer diameter of 4.2mm first, which has stronger attraction and can be sucked out. Later, a 3.0mm thin mirror can be used for deep drilling and exploration. If PCD, PBB, etc. are considered, and children are prone to a large amount of purulent secretions, it is also recommended to choose a thick mirror with an outer diameter of 4.2mm, which is easy to attract. In addition, a mirror with an outer diameter of 3.5mm can also be used.
For children aged 5 years or older and weighing 20 kg or more, a 4.2 mm outer diameter bronchoscope is generally preferred. A 2.0 mm forceps channel facilitates manipulation and suctioning.
However, a thinner 2.8/3.0 mm outer diameter bronchoscope should be selected in the following situations:
① Anatomical airway stenosis:
• Congenital or postoperative airway stenosis, tracheobronchomalacia, or extrinsic compression stenosis. • Internal diameter of the subglottic or narrowest bronchial segment < 5 mm.
② Recent airway trauma or edema
• Post-intubation glottic/subglottic edema, endotracheal burns, or inhalation injury.
③ Severe stridor or respiratory distress
• Acute laryngotracheobronchitis or severe status asthmaticus requiring minimal irritation.
④ Nasal route with narrow nasal openings
• Significant stenosis of the nasal vestibule or inferior turbinate during nasal insertion, preventing the passage of a 4.2 mm endoscope without injury.
⑤ Requirement to penetrate a peripheral (grade 8 or higher) bronchus.
• In some cases of severe Mycoplasma pneumonia with atelectasis, if multiple bronchoscopic alveolar lavages in the acute phase still fail to restore atelectasis, a fine endoscope may be needed to drill deeply into the distal bronchoscope to explore and treat small, deep sputum plugs. • In suspected cases of bronchial obstruction (BOB), a sequelae of severe pneumonia, a fine endoscope may be used to drill deeply into the subbranches and subsubbranches of the affected lung segment. • In cases of congenital bronchial atresia, deep drilling with a fine endoscope is also necessary for deep bronchial atresia. • In addition, some diffuse peripheral lesions (such as diffuse alveolar hemorrhage and peripheral nodules) require a finer endoscope.
⑥ Concomitant cervical or maxillofacial deformities
• Micromandibular or craniofacial syndromes (such as Pierre-Robin syndrome) restricting the oropharyngeal space.
⑦ Short procedure time, requiring only diagnostic examination
• Only BAL, brushing, or simple biopsy is required; no large instruments are required, and a thin endoscope can reduce irritation.
⑧ Postoperative follow-up
• Recent rigid bronchoscopy or balloon dilatation to minimize secondary mucosal trauma.
In short:
"Stenosis, edema, shortness of breath, small nares, deep periphery, deformity, short examination time, and postoperative recovery"—if any of these conditions are present, switch to a 2.8–3.0 mm thin endoscope.
4. For children aged >8 years and weighing >35 kg, an endoscope with an outer diameter of 4.9 mm or larger can be selected. However, for routine bronchoscopy, thinner endoscopes are less irritating to the patient and reduce the risk of complications unless specialized intervention is required.
5. Fujifilm's current primary pediatric EBUS model is the EB-530US. Its key specifications are as follows: distal outer diameter: 6.7 mm, insertion tube outer diameter: 6.3 mm, working channel: 2.0 mm, working length: 610 mm, and total length: 880 mm. Recommended age and weight: Due to the 6.7 mm distal diameter of the endoscope, it is recommended for children aged 12 years and older or weighing >40 kg.
Olympus Ultrasonic Bronchoscope: (1) Linear EBUS (BF-UC190F Series): ≥12 years old, ≥40 kg. (2) Radial EBUS + Ultrathin Mirror (BF-MP290F Series): ≥6 years old, ≥20 kg; for younger children, the probe and mirror diameters need to be further reduced.
Introduction to various bronchoscopy
Bronchoscopes are classified according to their structure and imaging principles into the following categories:
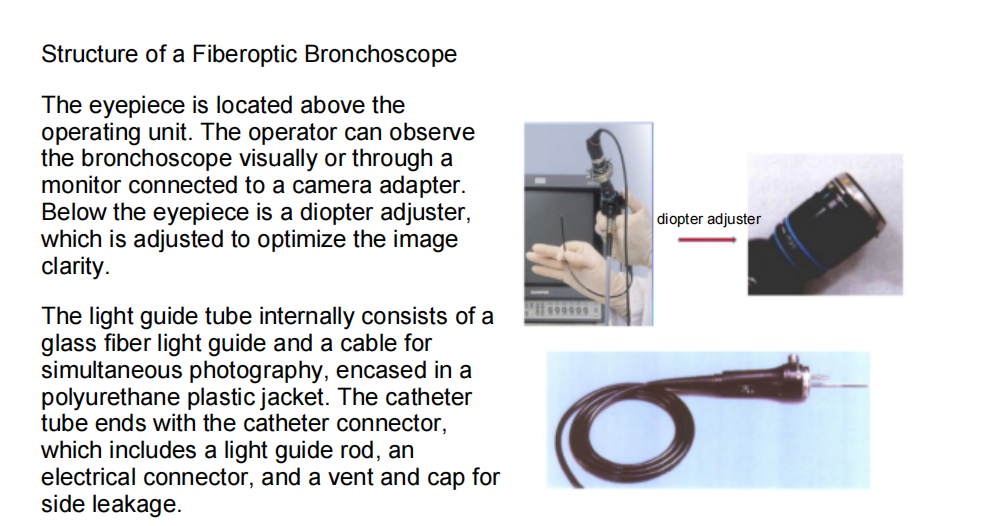
Fiberoptic bronchoscopes
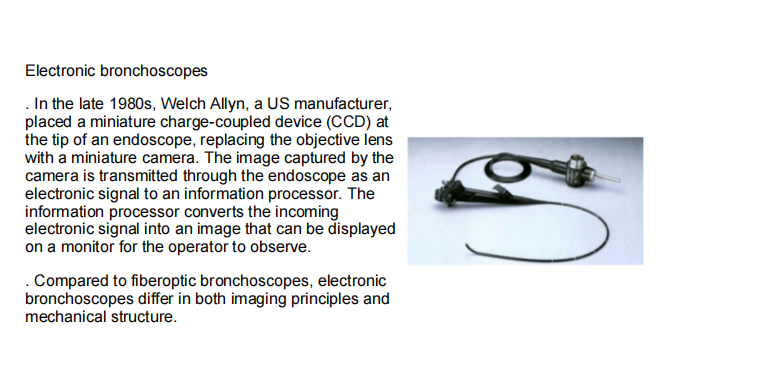
Electronic bronchoscopes
Combined bronchoscopes
Autofluorescence bronchoscopes
Ultrasound bronchoscopes
……
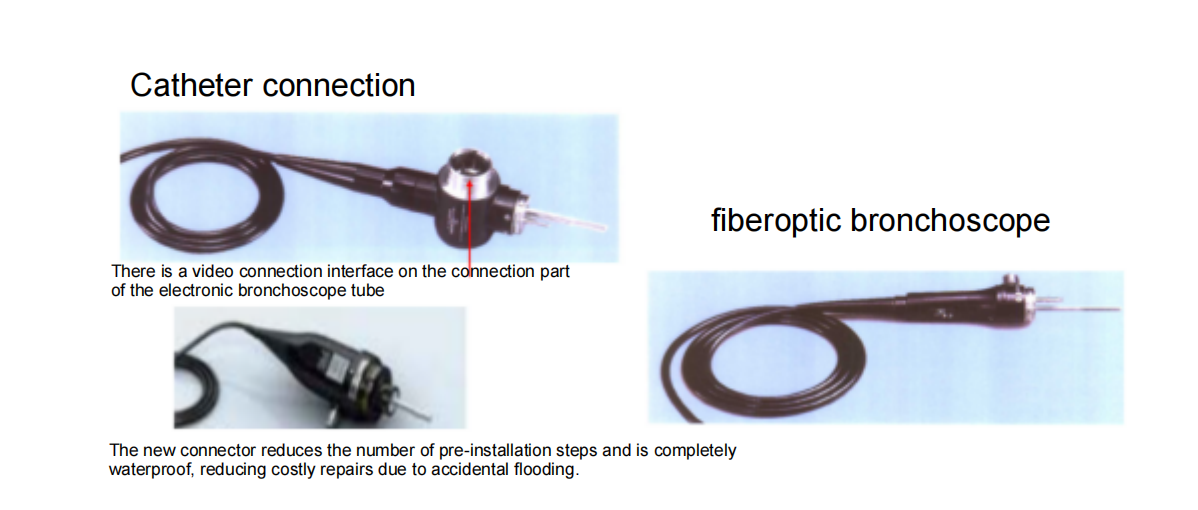
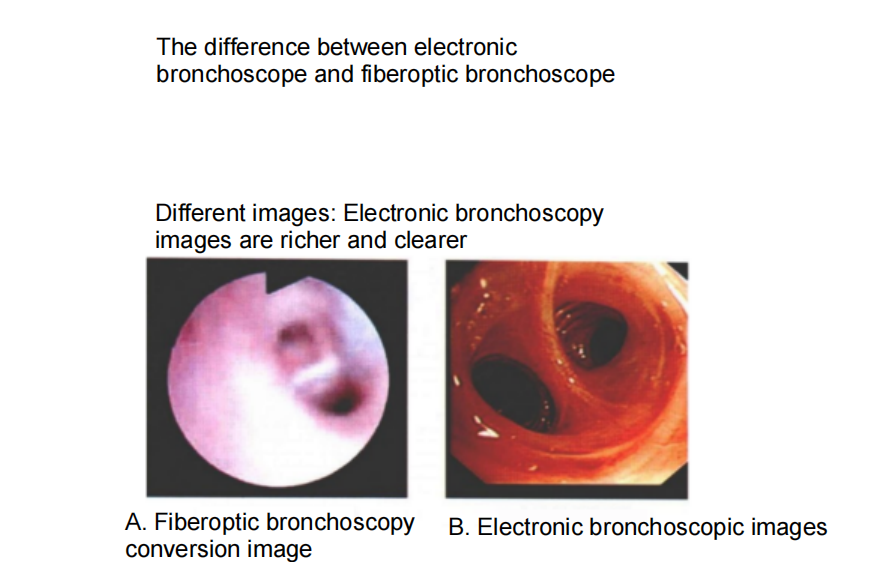
Fiberoptic bronchoscopy:
Electronic bronchoscope:
Compound bronchoscope:
Other bronchoscopes:
Ultrasound bronchoscopes (EBUS): An ultrasound probe integrated into the front end of an electronic endoscope is known as an "airway B-ultrasound." It can penetrate the airway wall and clearly visualize mediastinal lymph nodes, blood vessels, and tumors outside the trachea. It is particularly suitable for staging lung cancer patients. Through ultrasound-guided puncture, mediastinal lymph node samples can be accurately obtained to determine whether the tumor has metastasized, potentially avoiding the trauma of traditional thoracotomy. EBUS is divided into "large EBUS" for observing lesions around the large airways and "small EBUS" (with a peripheral probe) for observing peripheral lung lesions. The "large EBUS" clearly demonstrates the relationship between blood vessels, lymph nodes, and space-occupying lesions within the mediastinum outside the airways. It also allows for transbronchial needle aspiration directly into the lesion under real-time monitoring, effectively avoiding damage to surrounding large vessels and cardiac structures, improving safety and accuracy. The "small EBUS" has a smaller body, allowing it to clearly visualize peripheral lung lesions where conventional bronchoscopes cannot reach. When used with an introducer sheath, it allows for more precise sampling.
Fluorescence bronchoscopy: Immunofluorescence bronchoscopy combines conventional electronic bronchoscopes with cellular autofluorescence and information technology to identify lesions using the fluorescence differences between tumor cells and normal cells. Under specific wavelengths of light, precancerous lesions or early-stage tumors emit a unique fluorescence that differs from the color of normal tissue. This helps doctors detect tiny lesions that are difficult to detect with conventional endoscopy, thereby improving the early diagnosis rate of lung cancer.
Ultra-thin bronchoscopes: Ultra-thin bronchoscopes are a more flexible endoscopic technique with a smaller diameter (typically <3.0 mm). They are primarily used for precise examination or treatment of distal lung regions. Their key advantage lies in their ability to visualize subsegmental bronchi below level 7, enabling more detailed examination of subtle lesions. They can reach small bronchi that are difficult to reach with traditional bronchoscopes, improving the detection rate of early lesions and reducing surgical trauma.A cutting-edge pioneer in "navigation + robotics": exploring the "uncharted territory" of the lungs.
Electromagnetic navigation bronchoscopy (ENB) is like equipping a bronchoscope with a GPS. Preoperatively, a 3D lung model is reconstructed using CT scans. During surgery, electromagnetic positioning technology guides the endoscope through complex bronchial branches, precisely targeting small peripheral lung nodules measuring only a few millimeters in diameter (such as ground-glass nodules under 5 mm) for biopsy or ablation.
Robot-assisted bronchoscopy: The endoscope is controlled by a robotic arm operated by the physician at a console, eliminating the influence of hand tremors and achieving higher positioning accuracy. The end of the endoscope can rotate 360 degrees, allowing for flexible navigation through tortuous bronchial pathways. It is particularly well-suited for precise manipulation during complex lung surgeries and has already made a significant impact in the fields of small lung nodule biopsy and ablation.
Some domestic bronchoscopes:
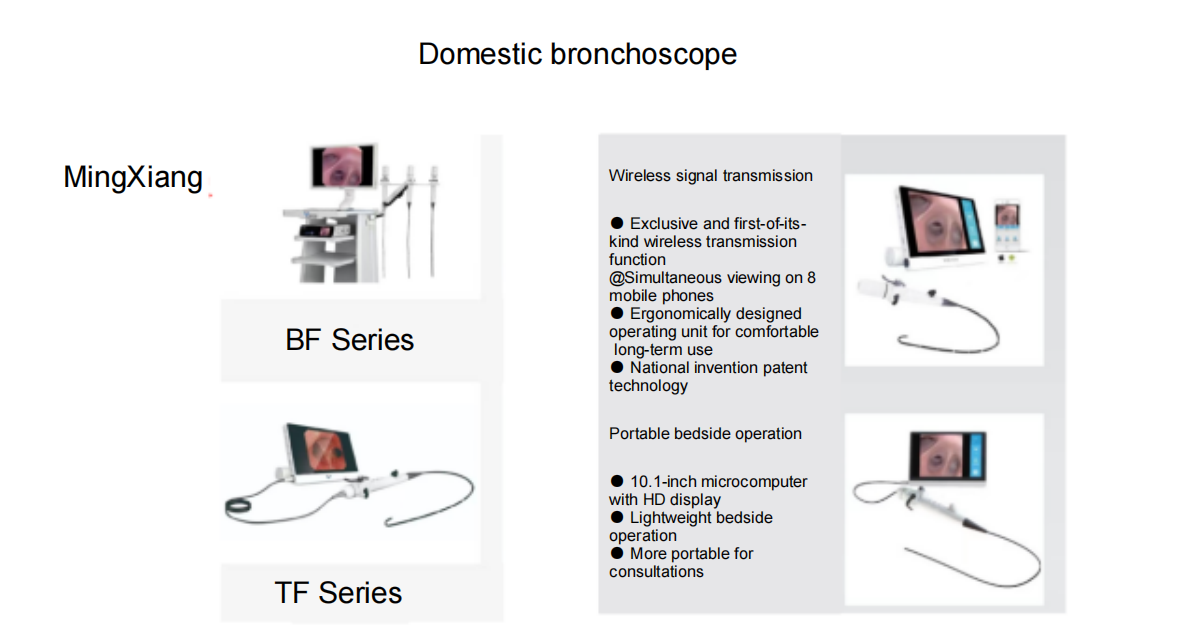
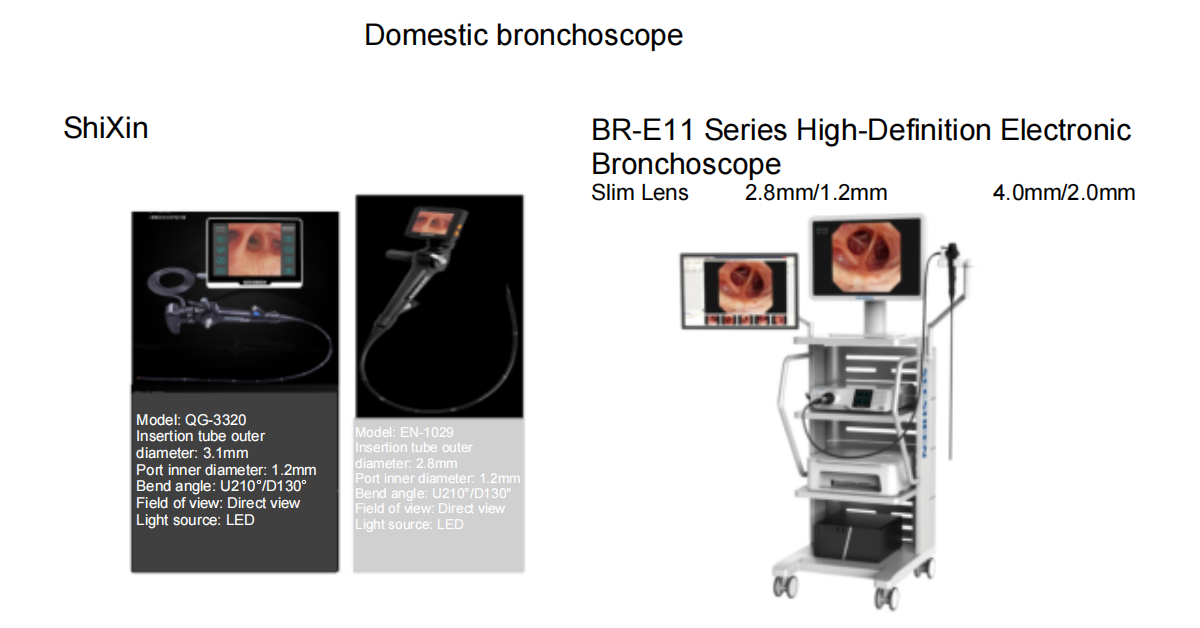
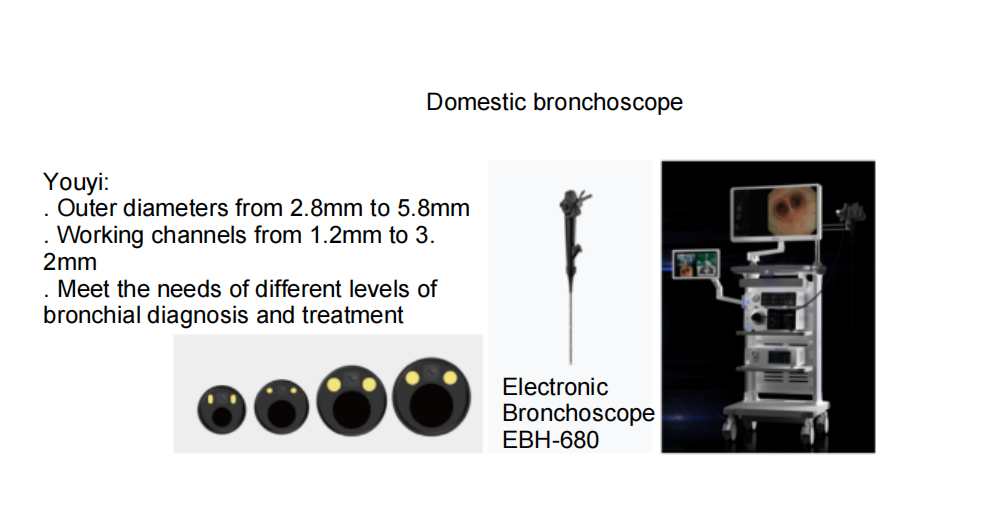
In addition, many domestic brands such as Aohua and Huaguang are also good.
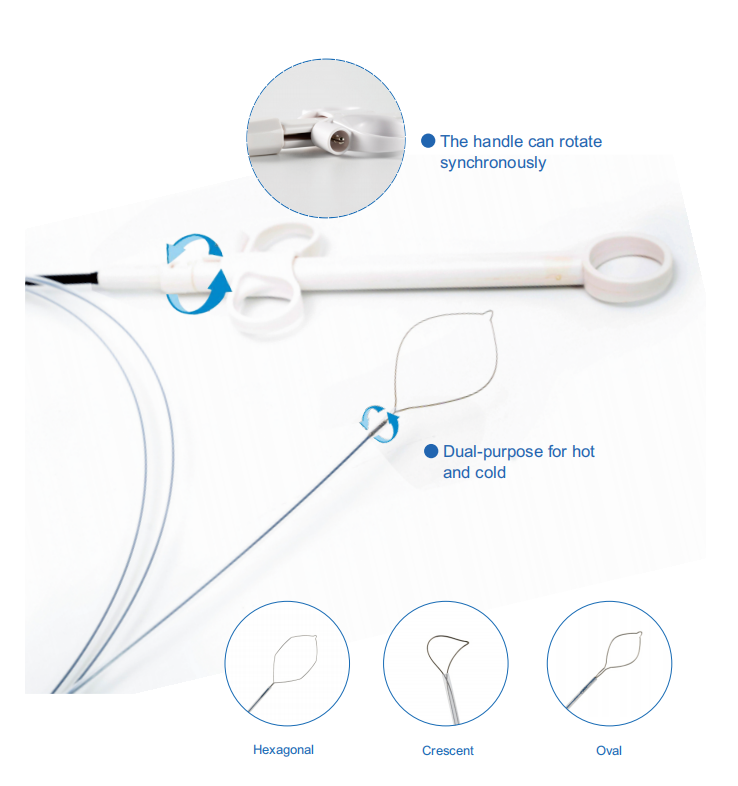
Let’s see what we can offer as bronchoscopy consumables
Here are our hot sell bronchoscopy compatible endoscopic consumables.
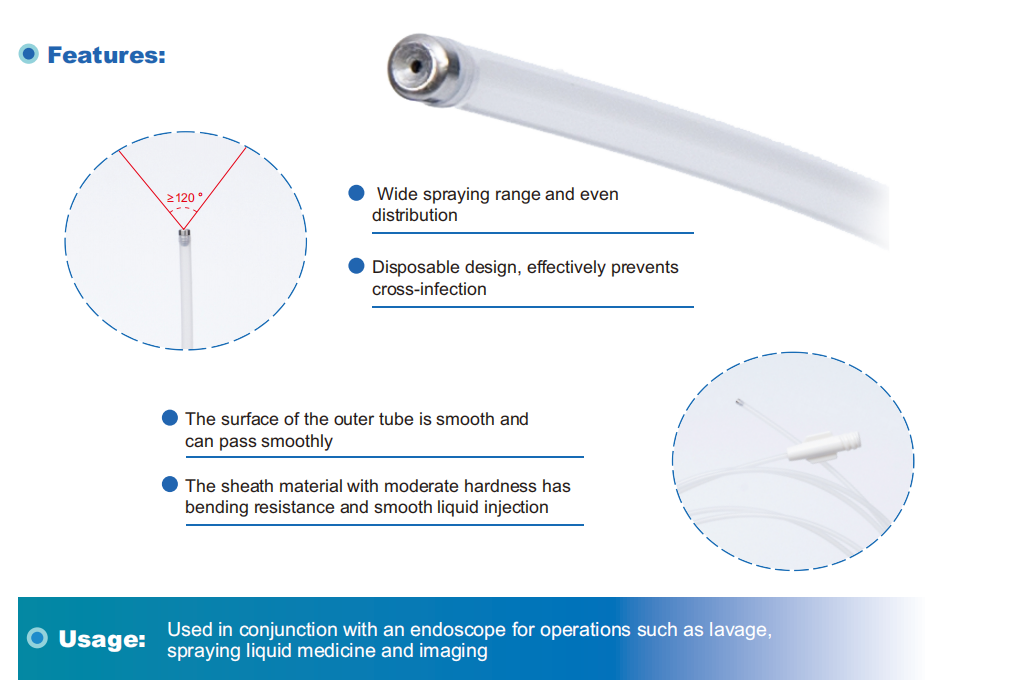
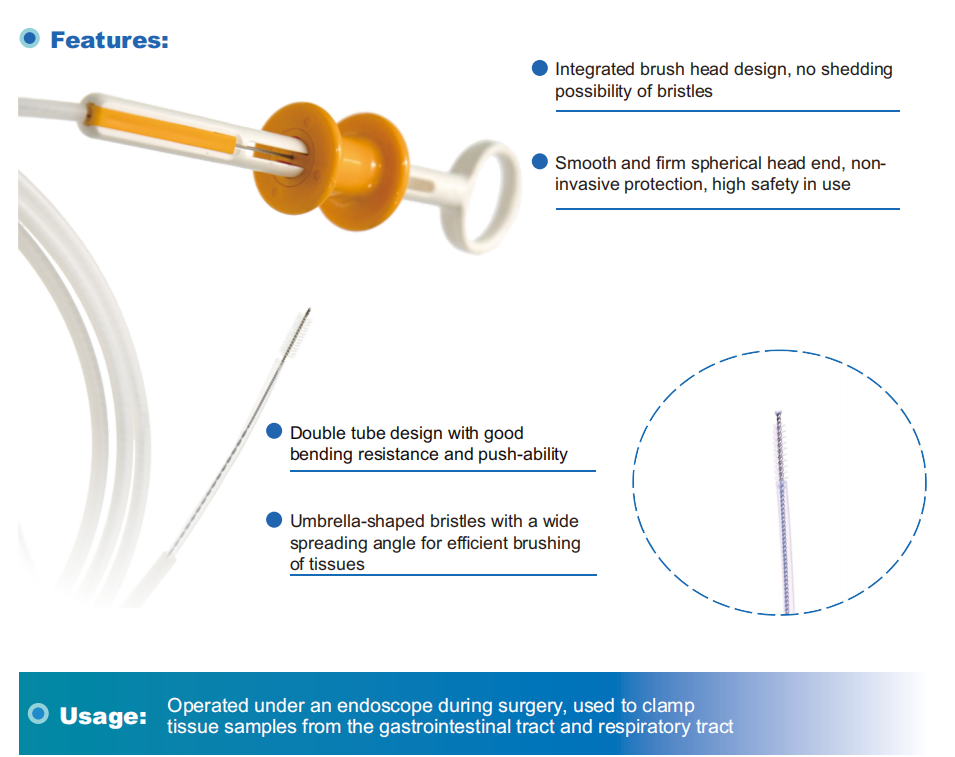
Disposable Biopsy Forceps-1.8mm biopsy forceps for reusable bronchoscopy

1.0mm biopsy forceps for disposable bronchoscopy

Post time: Sep-03-2025