

I.Patient preparation
1. Understand the location, nature, size and perforation of foreign objects
Take plain X-rays or CT scans of the neck, chest, anteroposterior and lateral views, or abdomen as needed to understand the location, nature, shape, size, and presence of perforation of the foreign body, but do not perform a barium swallow examination.
2. Fasting and water fasting time
Routinely, patients fast for 6 to 8 hours to empty the stomach contents, and the fasting and water fasting time can be appropriately relaxed for emergency gastroscopy.
3. Anesthesia assistance
Children, those with mental disorders, those who are uncooperative, or those with incarcerated foreign bodies, large foreign bodies, multiple foreign bodies, sharp foreign bodies, or endoscopic operations that are difficult or take a long time should be operated under general anesthesia or endotracheal intubation with the help of an anesthesiologist. Remove foreign objects.
II. Equipment preparation
1. Endoscope selection
All types of forward-viewing gastroscopy are available. If it is estimated that it is difficult to remove the foreign body or the foreign body is large, double-port surgical gastroscopy is used. Endoscopes with a smaller outer diameter can be used for infants and young children.
2. Selection of forceps
Mainly depends on the size and shape of the foreign body. Commonly used instruments include biopsy forceps, snare, three-jaw forceps, flat forceps, foreign body forceps (rat-tooth forceps, jaw-mouth forceps), stone removal basket, stone removal net bag, etc.
The choice of instrument can be determined based on the size, shape, type, etc. of the foreign body. According to literature reports, rat-tooth forceps are the most widely used. The usage rate of rat-tooth forceps is 24.0%~46.6% of all instruments used, and snares account for 4.0%~23.6%. It is generally believed that snares are better for long rod-shaped foreign bodies. Such as thermometers, toothbrushes, bamboo chopsticks, pens, spoons, etc., and the position of the end covered by the snare should not exceed 1cm, otherwise it will be difficult to exit the cardia.
2.1 Rod-shaped foreign bodies and spherical foreign bodies
For rod-shaped foreign objects with a smooth surface and a thin outer diameter such as toothpicks, it is more convenient to choose three-jaw pliers, rat-tooth pliers, flat pliers, etc.; for spherical foreign objects (such as cores, glass balls, button batteries, etc.), use a stone removal basket or a stone removal net bag to remove them Relatively difficult to slip off.
2.2 Long sharp foreign bodies, food clumps, and huge stones in the stomach
For long sharp foreign bodies, the long axis of the foreign body should be parallel to the longitudinal axis of the lumen, with the sharp end or open end facing downwards, and withdrawing while injecting air. For ring-shaped foreign bodies or foreign bodies with holes, it is safer to use the threading method to remove them;
For food clumps and huge stones in the stomach, bite forceps can be used to crush them and then be removed with three-jaw forceps or a snare.
3. Protective equipment
Use protective devices as much as possible for foreign objects that are difficult to remove and are risky. Currently, commonly used protective devices include transparent caps, outer tubes, and protective covers.
3.1 Transparent cap
During the foreign body removal operation, a transparent cap should be used at the end of the endoscopic lens as much as possible to prevent the mucosa from being scratched by the foreign body, and to expand the esophagus to reduce the resistance encountered when the foreign body is removed. It can also help to clamp and extract the foreign body, which is beneficial to the removal of the foreign body. take out.
For strip-shaped foreign bodies embedded in the mucosa at both ends of the esophagus, a transparent cap can be used to gently push the esophageal mucosa around one end of the foreign body so that one end of the foreign body exits the esophageal mucosal wall to avoid esophageal perforation caused by direct removal.
The transparent cap can also provide enough space for the operation of the instrument, which is convenient for the detection and removal of foreign bodies in the narrow esophageal neck segment.
At the same time, the transparent cap can use negative pressure suction to help absorb food clumps and facilitate subsequent processing.
3.2 Outer casing
While protecting the esophagus and the esophageal-gastric junction mucosa, the outer tube facilitates the endoscopic removal of long, sharp, and multiple foreign bodies and the removal of food clumps, thereby reducing the incidence of complications during upper gastrointestinal foreign body removal. Increase the safety and effectiveness of treatment.
Overtubes are not commonly used in children because of the risk of damaging the esophagus during insertion.
3.3 Protective cover
Place the protective cover upside down on the front end of the endoscope. After clamping the foreign object, flip the protective cover over and wrap the foreign object when withdrawing the endoscope to avoid foreign objects.
It comes into contact with the mucous membrane of the digestive tract and plays a protective role.
4. Treatment methods for different types of foreign bodies in the upper gastrointestinal tract
4.1 Food masses in esophagus
Reports suggest that most smaller food masses in the esophagus can be gently pushed into the stomach and left to be discharged naturally, which is simple, convenient and less likely to cause complications. During the gastroscopy advancement process, appropriate inflation can be introduced into the esophageal lumen, but some patients may be accompanied by esophageal malignant tumors or post-esophageal anastomotic stenosis (Figure 1). If there is resistance and you push violently, applying too much pressure will increase the risk of perforation. It is recommended to use a stone removal net basket or a stone removal net bag to directly remove the foreign body. If the food bolus is large, you can use foreign body forceps, snares, etc. to mash it up before dividing it. Take it out.
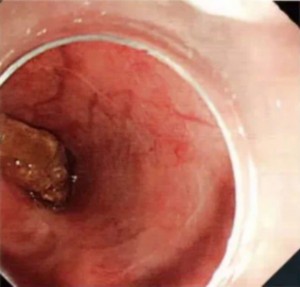
Figure 1 After surgery for esophageal cancer, the patient was accompanied by esophageal stenosis and food bolus retention.
4.2 Short and blunt foreign objects
Most short and blunt foreign bodies can be removed through foreign body forceps, snares, stone removal baskets, stone removal net bags, etc. (Figure 2). If the foreign body in the esophagus is difficult to remove directly, it can be pushed into the stomach to adjust its position and then try to remove it. Short, blunt foreign bodies with a diameter of >2.5 cm in the stomach are more difficult to pass through the pylorus, and endoscopic intervention should be performed as soon as possible; if foreign bodies with smaller diameters in the stomach or duodenum do not show gastrointestinal damage, they can wait for their natural discharge. If it remains for more than 3-4 weeks and still cannot be discharged, it must be removed endoscopically.
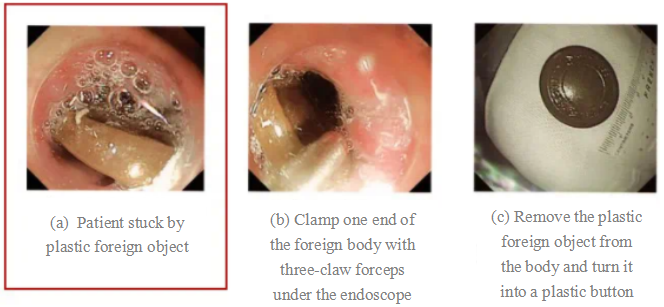
Figure 2 Plastic foreign objects and removal methods
4.3 Foreign bodies
Foreign objects with a length of ≥6 cm (such as thermometers, toothbrushes, bamboo chopsticks, pens, spoons, etc.) are not easy to be discharged naturally, so they are often collected with a snare or stone basket.
A snare can be used to cover one end (no more than 1 cm away from the end), and placed in a transparent cap to take it out. An outer cannula device can also be used to seize the foreign body and then retreat smoothly into the outer cannula to avoid damaging the mucosa.
4.4 Sharp foreign objects
Sharp foreign objects such as fish bones, poultry bones, dentures, date pits, toothpicks, paper clips, razor blades, and pill tin box wrappers (Figure 3) should be given sufficient attention. Sharp foreign objects that can easily damage mucous membranes and blood vessels and lead to complications such as perforation should be treated carefully. Emergency endoscopic management.
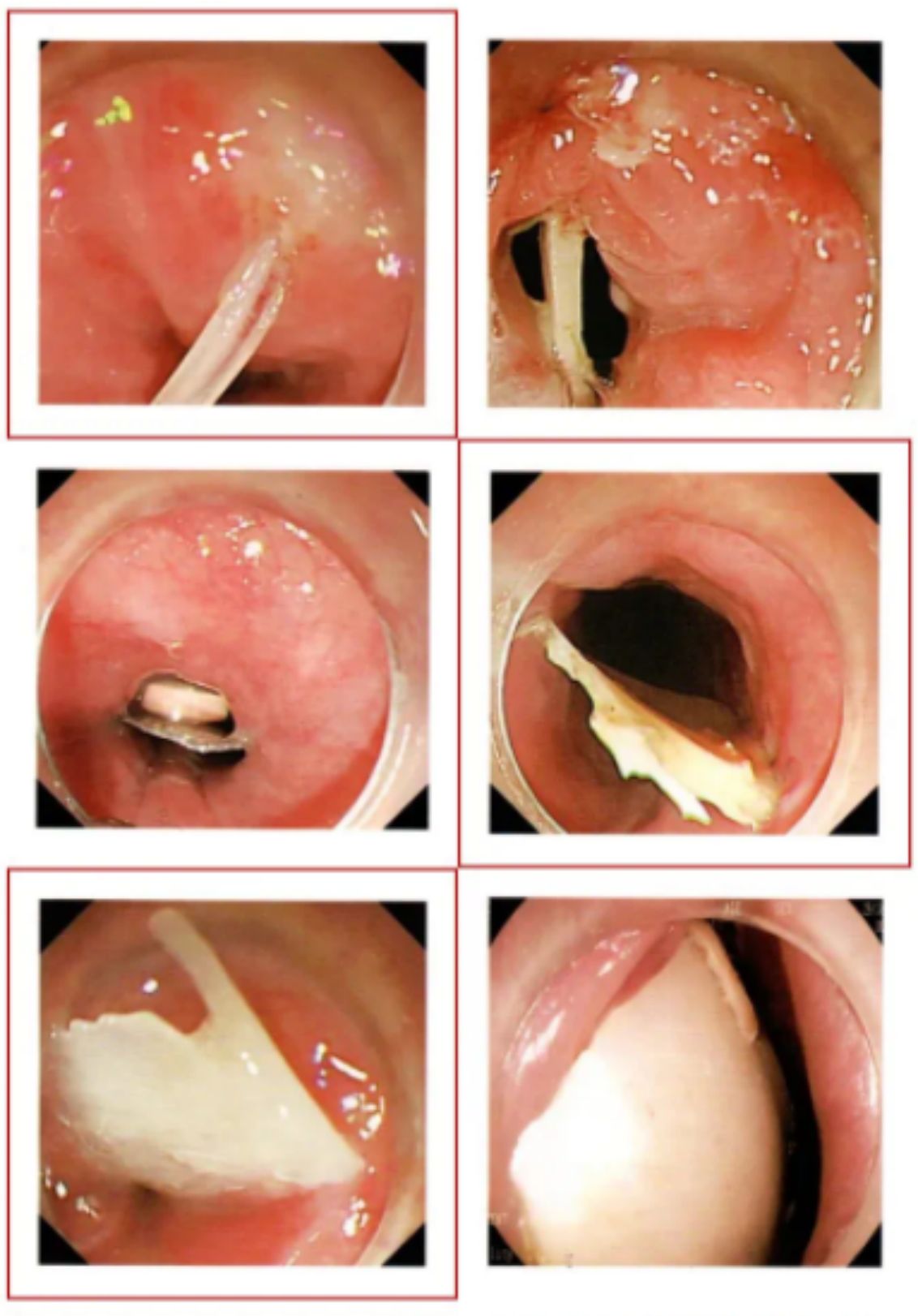
Figure 3 Different types of sharp foreign objects
When removing sharp foreign bodies under an endoscope, it is easy to scratch the mucosa of the digestive tract. It is recommended to use a transparent cap, which can fully expose the lumen and avoid scratching the wall. Try to bring the blunt end of the foreign body close to the end of the endoscopic lens so that one end of the foreign body is placed Put it into the transparent cap, use foreign body forceps or a snare to grasp the foreign body, and then try to keep the longitudinal axis of the foreign body parallel to the esophagus before withdrawing from the scope. Foreign bodies embedded in one side of the esophagus can be removed by placing a transparent cap on the front end of the endoscope and slowly entering the esophageal inlet. For foreign bodies embedded in the esophageal cavity at both ends, the shallower embedded end should be loosened first, usually On the proximal side, pull out the other end, adjust the direction of the foreign object so that the head end is included in the transparent cap, and take it out. Or after using a laser knife to cut the foreign body in the middle, our experience is to loosen the aortic arch or heart side first, and then remove it in stages.
a.Dentures: When eating, coughing, or talking, patients may accidentally fall off their dentures, and then enter the upper gastrointestinal tract with swallowing movements. Sharp dentures with metal clasps at both ends are easy to become embedded in the walls of the digestive tract, making removal difficult. For patients who fail conventional endoscopic treatment, multiple clamping instruments can be used to attempt removal under dual-channel endoscopy.
b.Date pits: Date pits embedded in the esophagus are usually sharp at both ends, which can lead to complications such as mucosal damage, bleeding, local suppurative infection and perforation in a short period of time, and should be treated with emergency endoscopic treatment (Figure 4). If there is no gastrointestinal injury, most of the date stones in the stomach or duodenum can be excreted within 48 hours. Those who cannot be excreted naturally should be removed as soon as possible.
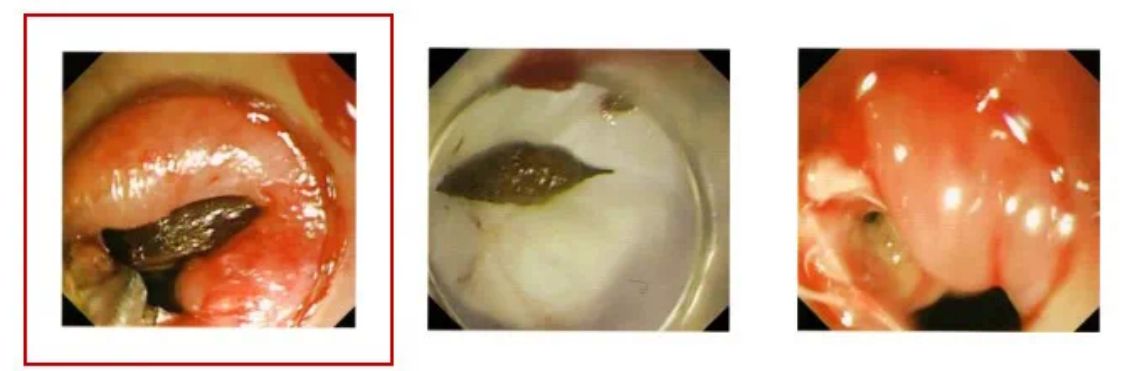
Figure 4 Jujube core
Four days later, the patient was diagnosed with a foreign body in another hospital. CT showed a foreign body in the esophagus with perforation. The sharp jujube cores at both ends were removed under endoscopy and the gastroscopy was performed again. It was found that a fistula was formed on the wall of the esophagus.
4.5 Larger foreign objects with long edges and sharp edges (Figure 5)
a. Install the outer tube under endoscope: Insert the gastroscope from the center of the outer tube, so that the lower edge of the outer tube is close to the upper edge of the curved part of the gastroscope. Routinely insert the gastroscope near the foreign body. Insert appropriate instruments through the biopsy tube, such as snares, foreign body forceps, etc. After grabbing the foreign object, put it into the outer tube, and the entire device will exit together with the mirror.
b. Homemade mucous membrane protective cover: Use the thumb cover of medical rubber gloves to make a homemade endoscope front-end protective cover. Cut it along the bevel of the thumb root of the glove into a trumpet shape. Cut a small hole at the fingertip, and pass the front end of the mirror body through the small hole. Use a small rubber ring to fix it 1.0cm away from the front end of the gastroscope, put it back into the upper end of the gastroscope, and send it along with the gastroscope to the foreign body. Grab the foreign body and then withdraw it together with the gastroscope. The protective sleeve will naturally move towards the foreign body due to resistance. If the direction is reversed, it will be wrapped around foreign objects for protection.

Figure 5: Sharp fish bones were removed endoscopically, with mucosal scratches
4.6 Metallic foreign matter
In addition to conventional forceps, metallic foreign bodies can be removed by suction with magnetic foreign body forceps. Metallic foreign bodies that are more dangerous or difficult to remove can be treated endoscopically under X-ray fluoroscopy. It is recommended to use a stone removal basket or a stone removal net bag.
Coins are more common among foreign bodies in the digestive tract of children (Figure 6). Although most coins in the esophagus can be passed naturally, elective endoscopic treatment is recommended. Because children are less cooperative, endoscopic removal of foreign bodies in children is best performed under general anesthesia. If the coin is difficult to remove, it can be pushed into the stomach and then taken out. If there are no symptoms in the stomach, you can wait for it to be excreted naturally. If the coin remains for more than 3-4 weeks and is not expelled, it must be treated endoscopically.
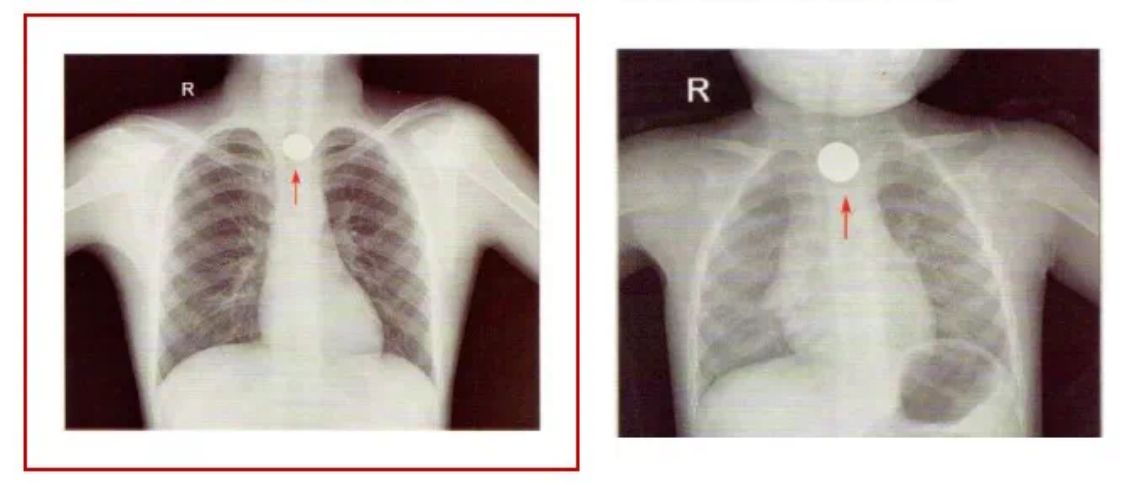
Figure 6 Metal coin foreign matter
4.7 Corrosive foreign matter
Corrosive foreign bodies can easily cause damage to the digestive tract or even necrosis. Emergency endoscopic treatment is required after diagnosis. Batteries are the most common corrosive foreign body and often occur in children under 5 years old (Figure 7). After damaging the esophagus, they may cause esophageal stenosis. Endoscopy must be reviewed within a few weeks. If stricture is formed, the esophagus should be dilated as soon as possible.
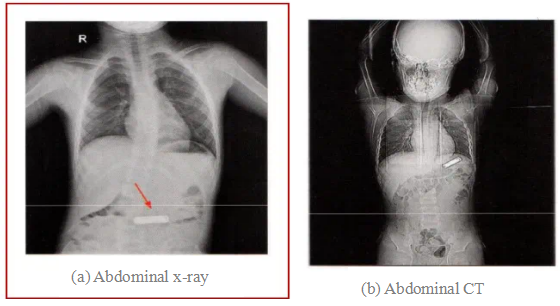
Figure 7 Foreign object in the battery, the red arrow indicates the location of the foreign object
4.8 Magnetic foreign matter
When multiple magnetic foreign bodies or magnetic foreign bodies combined with metal are present in the upper gastrointestinal tract, the objects attract each other and compress the walls of the digestive tract, which can easily cause ischemic necrosis, fistula formation, perforation, obstruction, peritonitis and other serious gastrointestinal injuries. , requiring emergency endoscopic treatment. Single magnetic foreign objects should also be removed as soon as possible. In addition to conventional forceps, magnetic foreign bodies can be removed under suction with magnetic foreign body forceps.
4.9 Foreign bodies in the stomach
Most of them are lighters, iron wires, nails, etc. that are deliberately swallowed by prisoners. Most foreign bodies are long and large, difficult to pass through the cardia, and can easily scratch the mucous membrane. It is recommended to use condoms combined with rat-tooth forceps to remove foreign bodies under endoscopic examination. First, insert the rat-tooth forceps into the front end of the endoscope through the endoscopic biopsy hole. Use the rat-tooth forceps to clamp the rubber ring at the bottom of the condom. Then, retract the rat-tooth forceps toward the biopsy hole so that the length of the condom is exposed outside the biopsy hole. Minimize it as much as possible without affecting the field of view, and then insert it into the gastric cavity along with the endoscope. After discovering the foreign body, put the foreign body into the condom. If it is difficult to remove, place the condom in the gastric cavity, and use rat-tooth forceps to clamp the foreign body and put it in. Inside the condom, use rat-tooth pliers to clamp the condom and withdraw it together with the mirror.
4.10 Stomach stones
Gastroliths are divided into vegetable gastroliths, animal gastroliths, drug-induced gastroliths and mixed gastroliths. Vegetative gastroliths are the most common, mostly caused by eating a large amount of persimmons, hawthorns, winter dates, peaches, celery, kelp, and coconuts on an empty stomach. Caused by etc. Plant-based gastroliths such as persimmons, hawthorns, and jujubes contain tannic acid, pectin, and gum. Under the action of gastric acid, water-insoluble tannic acid protein is formed, which binds to pectin, gum, plant fiber, peel, and core. Stomach stones.
Gastric stones exert mechanical pressure on the stomach wall and stimulate increased gastric acid secretion, which can easily cause gastric mucosal erosion, ulcers and even perforation. Small, soft gastric stones can be dissolved with sodium bicarbonate and other drugs and then allowed to be excreted naturally.
For patients who fail medical treatment, endoscopic stone removal is the first choice (Figure 8). For gastric stones that are difficult to remove directly under endoscopy due to their large size, foreign body forceps, snares, stone removal baskets, etc. can be used to directly crush the stones and then remove them; for those with hard texture that cannot be crushed, endoscopic cutting of the stones can be considered , Laser lithotripsy or high-frequency electric lithotripsy treatment, when the gastric stone is less than 2cm after being broken, use three-claw forceps or foreign body forceps to remove it as much as possible. Care should be taken to prevent stones larger than 2cm from being discharged into the intestinal cavity through the stomach and causing intestinal obstruction.

Figure 8 Stones in the stomach
4.11 Drug Bag
The rupture of the drug bag will pose a fatal risk and is a contraindication for endoscopic treatment. Patients who are unable to discharge naturally or who are suspected of having a drug bag rupture should actively undergo surgery.
III. Complications and treatment
The complications of the foreign body are related to the nature, shape, residence time and the doctor's operating level. The main complications include esophageal mucosal injury, bleeding, and perforation infection.
If the foreign body is small and there is no obvious mucosal damage when taken out, hospitalization is not required after the operation, and a soft diet can be followed after fasting for 6 hours. For patients with esophageal mucosal injuries, glutamine granules, aluminum phosphate gel and other mucosal protective agents can be given symptomatic treatment. If necessary, fasting and peripheral nutrition can be given.
For patients with obvious mucosal damage and bleeding, treatment can be performed under direct endoscopic vision, such as spraying ice-cold saline norepinephrine solution, or endoscopic titanium clips to close the wound.
For patients whose preoperative CT suggests that the foreign body has penetrated the esophageal wall after endoscopic removal, if the foreign body remains for less than 24 hours and CT finds no abscess formation outside the esophageal lumen, endoscopic treatment can be performed directly. After the foreign body is removed through the endoscope, a titanium clip is used to clamp the inner wall of the esophagus at the perforation site, which can stop bleeding and close the inner wall of the esophagus at the same time. A gastric tube and a jejunal feeding tube are placed under direct vision of the endoscope, and the patient is hospitalized for continued treatment. Treatment includes symptomatic treatment such as fasting, gastrointestinal decompression, antibiotics and nutrition. At the same time, vital signs such as body temperature must be closely observed, and the occurrence of complications such as neck subcutaneous emphysema or mediastinal emphysema must be observed on the third day after surgery. After iodine water angiography shows that there is no leakage, eating and drinking can be allowed.
If the foreign body has been retained for more than 24 hours, if infection symptoms such as fever, chills, and significantly elevated white blood cell count occur, if CT shows the formation of an extraluminal abscess in the esophagus, or if serious complications have occurred, patients should be transferred to surgery for treatment in a timely manner.
IV. Precautions
(1) The longer the foreign body stays in the esophagus, the more difficult the operation will be and the more complications will occur. Therefore, emergency endoscopic intervention is particularly necessary.
(2) If the foreign body is large, irregular in shape or has spikes, especially if the foreign body is in the middle of the esophagus and close to the aortic arch, and it is difficult to remove it endoscopically, do not forcefully pull it out. It is better to seek multidisciplinary consultation and preparation for surgery.
(3) Rational use of esophageal protection devices can reduce the occurrence of complications.
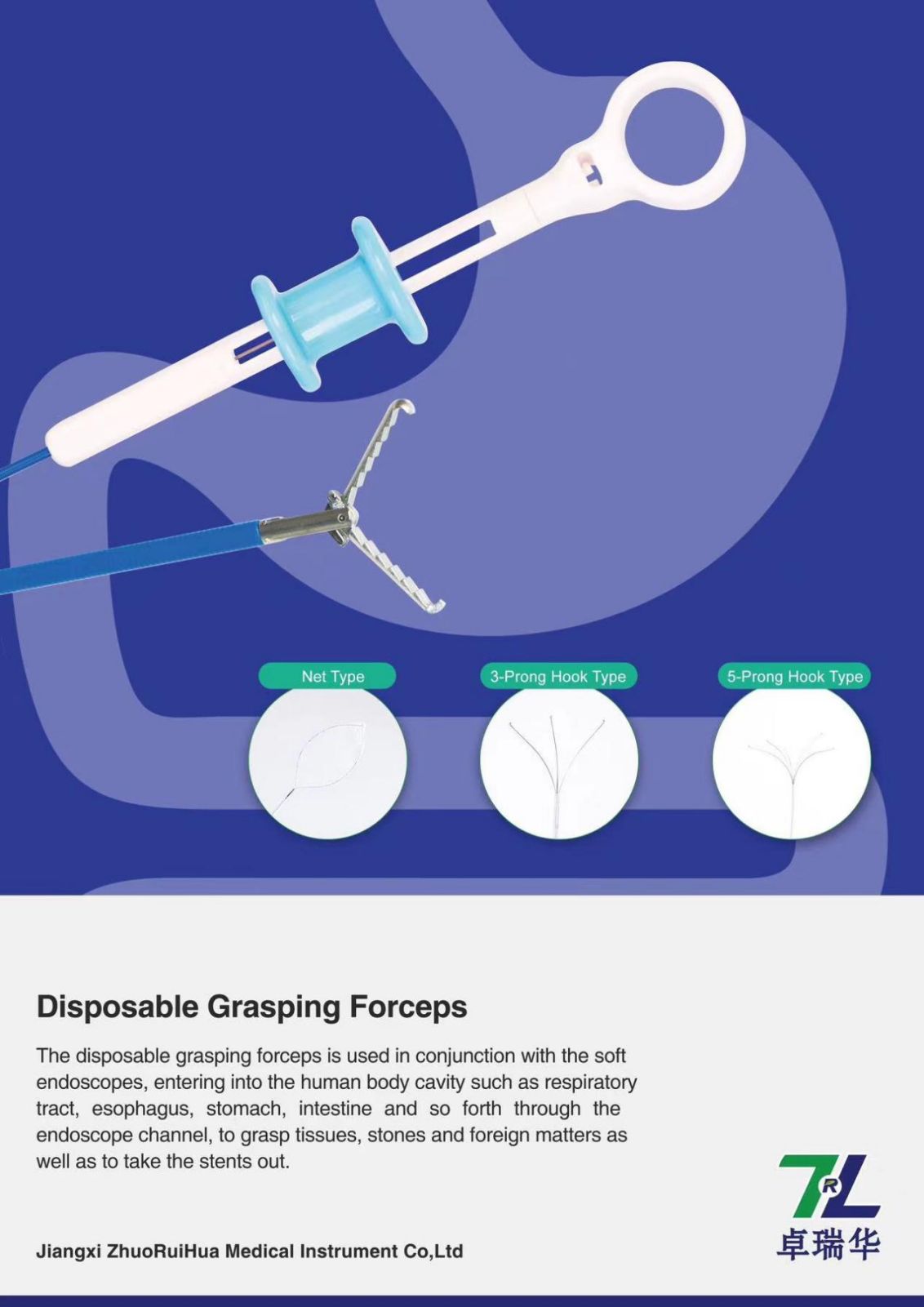
Our disposable grasping forceps is used in conjunction with the soft endoscopes, entering into the human body cavity such as respiratory tract, esophagus,stomach, intestine and so forth through the endoscope channel, to grasp tissues, stones and foreign matters as well as to take the stents out.

Post time: Jan-26-2024