

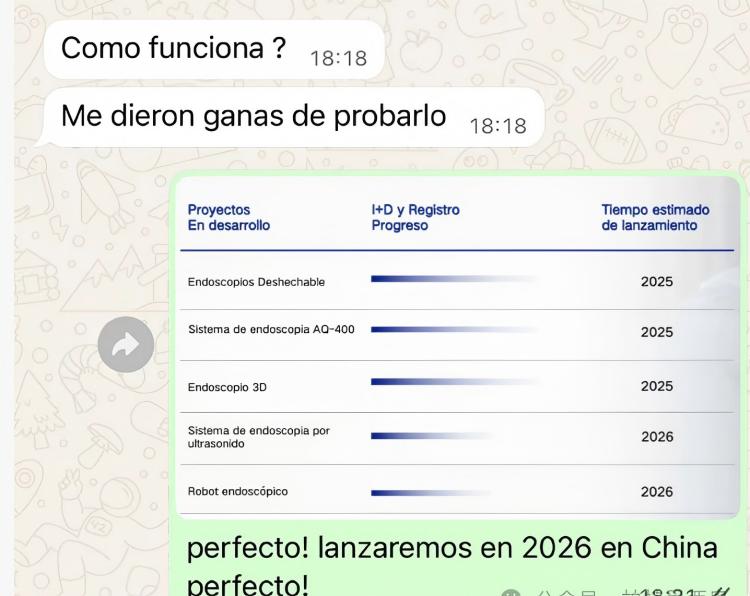
Latin American doctors are thrilled that ERCP has entered a new era of robotic surgery and are spreading the news far and wide.
During a recent conversation with doctors in Latin America, I mentioned the ERCP surgical robot from Ausway Endoscopy, which is currently undergoing clinical trials. When they learned that this system can perform robot-assisted ERCP, remotely controlling the flexible endoscope and instruments via a robotic arm to complete procedures such as biliary stent placement without wearing lead aprons and with significantly reduced radiation exposure, the atmosphere instantly became electric. Many doctors were so excited that they were practically spreading the news.


In my spare time, I wondered: why were they so excited?
With this question in mind, I reviewed the relevant literature and data again, and the more I read, the clearer it became—ERCP surgical robots are truly a godsend for endoscopists, even a life-changing technology.
Below, I'd like to share with you: The Silent Killer in Endoscopy: A Radiation Crisis Closer Than You Think! Everyone Performing ERCP Must Read This
The most easily overlooked thing in the operating room isn't complications, but the beam of light that's quietly accumulating.
Many endoscopists know that ERCP uses fluoroscopy, but you might not know—This procedure has been listed by the FDA as a high-risk examination that "may cause serious radiation damage."
We're busy treating gallstones and strictures, but we often overlook something even more terrifying:
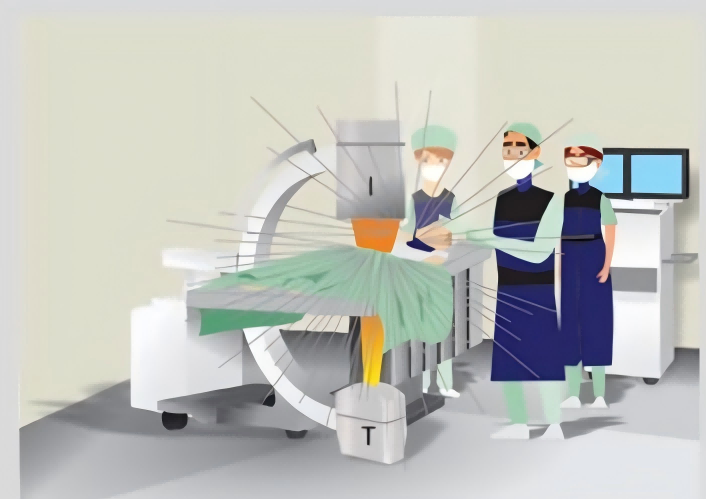
Radiation is quietly harming patients, and it harms everyone standing next to the C-arm.
Today, in the easiest-to-understand way, I'll explain international guidelines and real research data:
How much are you actually exposed to? What habits are "stealing" your health? How can you truly ensure safety?
I. Why is ERCP considered a high-risk procedure involving radiation?
Because ERCP meets all the conditions for "high-dose exposure"
● Requires fluoroscopy
● Complex procedure
● Close proximity to the doctor
● Long duration
● Repetitive procedures
How alarming are the real figures?
The radiation dose of one ERCP procedure is approximately equivalent to 312 chest X-rays (average).
—A study from an ERCP radiation measurement project in Uruguay
More importantly: You make dozens, hundreds, or even more a year.
II. What effects does radiation actually have on you?
Radiation damage is classified into two categories:
1) Deterministic damage (will occur if the dose is sufficient)
● Redness of the skin
● Hair loss
● Desquamation
● Ulcers
● Cataracts (prone to long-term accumulation of toxic substances)
The lens is one of the most fragile organs, and ICRP has lowered the threshold to 20 mSv/year.
Many ERCP specialists who have worked for over a decade have already experienced lens opacity.
2) Random damage (probabilistic damage)
There is no threshold.
The higher the dose, the greater the risk.
ICRP estimate: 1 mSv = 0.005% increase in lifetime cancer risk. One ERCP ≈ 6 mSv → 0.03% increase in risk.
You're not doing it "once".
You're doing it dozens of times a year, thousands of times in your lifetime.
III. The most dangerous spot in the ERCP room is actually where you stand every day.
In short: The closer to the X-ray tube, the higher the dose.
High-risk areas for personnel exposure include:
● One side of the C-arm X-ray tube
● During oblique angle imaging
● The area around the patient (the largest source of scattered radiation)
● The positions where anesthesiologists and nurses are stationed
Many people don't know that: The positions they stand in are the highest points of radiation exposure.

IV. Real Investigation: 90% of Medical Staff Did Not Take Proper Protective Measures
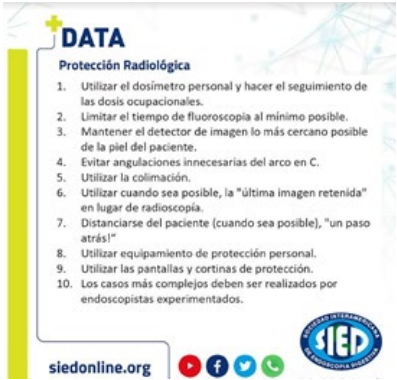
The findings of the Sociedad Interamericana de Endoscopía Digestiva (SIED) survey are quite astonishing:
● Only 22% of doctors have received radiation protection training.
● Only 17% of nurses have received training.
● Besides lead aprons, the usage rate of other protective equipment is extremely low.
Do you consider yourself "safe"? The reality is: Most people are running around naked.
V. The ALARA Principle: 3 Rules Everyone Must Follow
ALARA = As Low As Reasonably Achievable
1.Time: As short as possible.
● Pulse fluoroscopy
● Use "Frozen Last Frame"
● Prevent continuous fluoroscopy
2.Distance: The farther the better. With each step back, the dosage → becomes 1/4 of the original.
3.Shielding: Block as much as possible.
● Lead apron (≥0.35 mmPb)
● Thyroid protection
● Lead glasses (for cataract prevention)
● Lead curtains
● Suspended screens
A lead curtain can reduce scattered radiation by more than 95%.

VI. Where are the real risks for patients?
High BMI, repeated ERCP, high contrast doses, long procedure times. These can all lead to rapid accumulation of skin dose in patients.
Special attention:
● Women
● Pregnant women
● Children (sensitivity ×3–5)
● Repeated irradiation of the same area
These patients must have strictly limited doses.
VII. Pregnant Women and Children: High-Risk Groups That Must Be Discussed Separately.
ERCP Principles for Pregnant Women
● Is it "truly necessary"?
● Can it be postponed?
● Is it performed by the most experienced doctor?
● Is the fluoroscopy time minimized to the maximum extent?
● The most dangerous period of pregnancy (10–25 weeks).
ERCP principles for children
● Extremely high agent sensitivity.
● strict light and collimation control is essential.
● Only highly experienced operators are permitted.
VIII. Five things a truly professional ERCP room must do:
1. Dual dosimeter system (standard): One outside the lead apron, one inside.
2. Establish DRL (Diagnostic Reference Level): Japan's latest DRL: 32 Gy·cm² (75th percentile).
3. Inspect lead aprons annually (you'll be shocked by their breakage rate).
4. Provide patients with radiation information sheets (standard practice in well-managed departments).
5. Follow up high-dose patients for 2–4 weeks (skin damage may be delayed).
In conclusion: Protecting yourself is the only way to protect more patients.
The radiation you are exposed to is: invisible, painless, and doesn't cause redness, you don't feel it immediately, but it accumulates and harms you every day.
Learn proper protection so you can:
● Work longer
● Work more safely
● Work healthier
● Work more professionally
May every ERCP doctor be under the light, but never be harmed by it.
ERCP Series hot sell items from ZRHmed.
 |
 |
 |
 |
| Sphincterotome | Nonvascular Guidewires | Disposable Stone Retrieval Baskets | Disposable Nasobiliary Catheters |
We, Jiangxi Zhuoruihua Medical Instrument Co.,Ltd., is a manufacturer in China specializing in the endoscopic consumables, include GI line such as biopsy forceps, hemoclip, polyp snare, sclerotherapy needle, spray catheter, cytology brushes, guidewire, stone retrieval basket, nasal biliary drainage cathete etc. which are widely used in EMR, ESD, ERCP. Our products are CE certified and with FDA 510K approval, and our plants are ISO certified. Our goods have been exported to Europe, North America, Middle East and part of Asia, and widely obtains the customer of the recognition and praise!

Post time: Jan-13-2026