
In colonoscopic treatment, representative complications are perforation and bleeding.
Perforation refers to a state in which the cavity is freely connected to the body cavity due to a full-thickness tissue defect, and the presence of free air on X-ray examination does not affect its definition.
When the periphery of the full-thickness tissue defect is covered and has no free communication with the body cavity, it is called a perforation.
The definition of bleeding is not well-defined; current recommendations include a decrease in hemoglobin greater than 2 g/dL or the need for transfusion.
Postoperative bleeding is usually defined as the occurrence of significant blood in the stool after surgery that requires hemostatic treatment or blood transfusion.
The incidence of these incidental events varies with treatment:
Perforation rate:
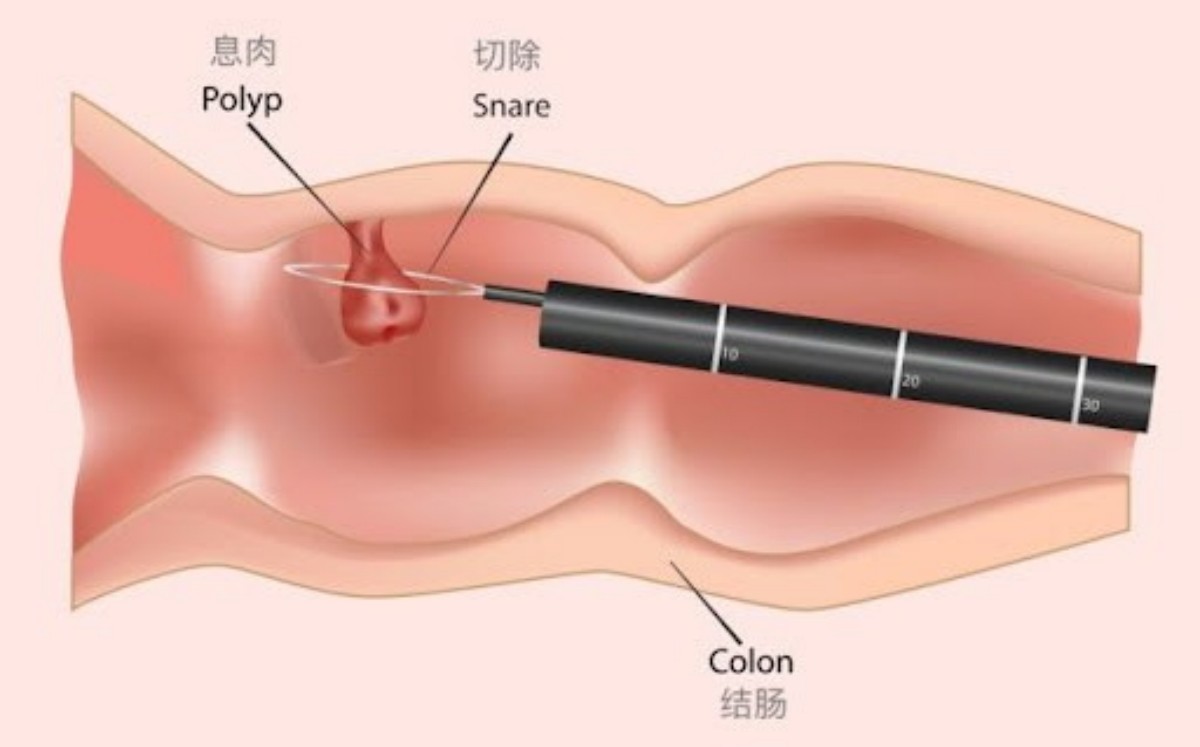
Polypectomy: 0.05%
Endoscopic mucosal resection (EMR): 0.58%~0.8%
Endoscopic submucosal dissection (ESD): 2%~14%
Postoperative bleeding rate:
Polypectomy: 1.6%
EMR : 1.1%~1.7%
ESD : 0.7%~3.1
1. How to deal with perforation
Since the wall of the large intestine is thinner than that of the stomach, the risk of perforation is higher. Adequate preparation is required before surgery to deal with the possibility of perforation.
Intraoperative precautions:
Ensure good operability of the endoscope.
Select appropriate endoscopes, treatment instruments, injection fluids and carbon dioxide gas delivery equipment according to the location, morphology and degree of fibrosis of the tumor.
Management of intraoperative perforation:
Immediate closure: Regardless of the location, clip closure is the preferred method (recommendation strength: Grade 1, evidence level: C).
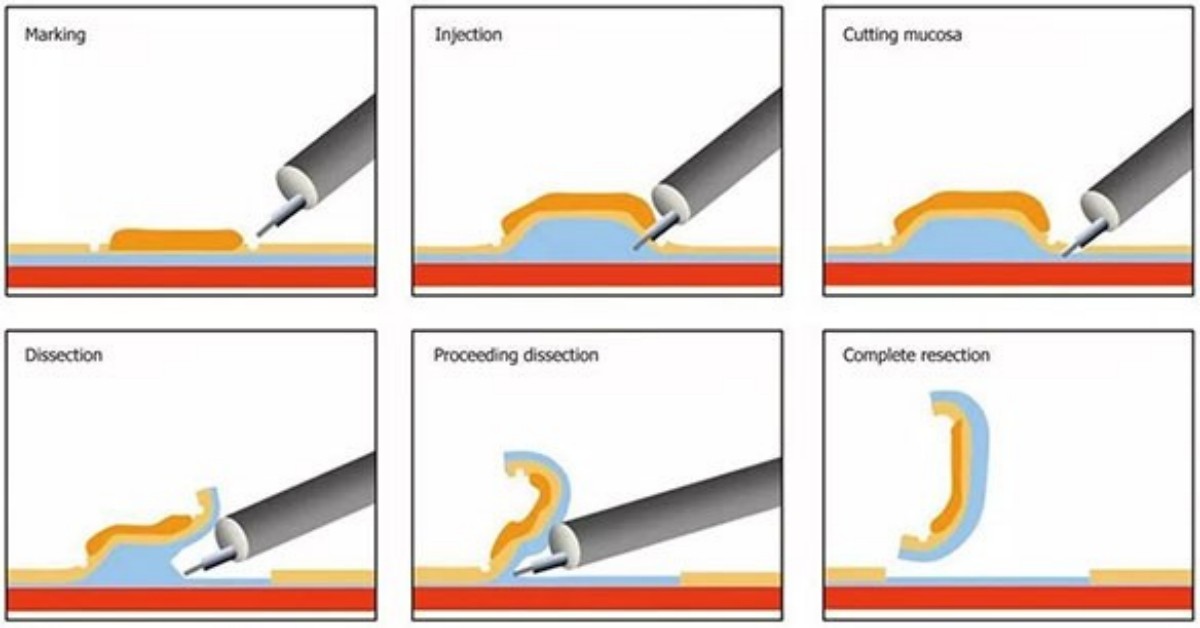
In ESD , in order to avoid interference with the dissection operation, the surrounding tissue should be dissected first to ensure sufficient operating space before closing.
Postoperative observation: If the perforation can be completely closed, surgery can be avoided by only antibiotic treatment and fasting.
Surgical decision: The need for surgery is determined based on a combination of abdominal symptoms, blood test results, and imaging rather than solely on free gas shown on CT.
Special parts treatment:
The lower rectum will not cause abdominal perforation due to its anatomical characteristics, but it may cause pelvic perforation, manifesting as retroperitoneal, mediastinal, or subcutaneous emphysema.
Precautions:
Postoperative wound closure may prevent complications to a certain extent, but there is insufficient evidence to show that it can effectively prevent delayed perforation.
2. Response to Bleeding
Management of intraoperative bleeding:
Use heat coagulation or hemostatic clips to stop bleeding.
Small vessel bleeding:
EMR , the snare tip can be used for thermal coagulation.
ESD , the tip of the electric knife can be used to contact thermal coagulation or hemostatic forceps to stop bleeding.
Large vessel bleeding: Use hemostatic forceps, but control the range of coagulation to avoid delayed perforation.
Prevention of postoperative bleeding:
Wound resection after EMR :
Studies have shown that the use of hemostatic forceps for preventive coagulation has no significant effect on postoperative bleeding rates, but there is a trend towards a decrease.
Prophylactic clipping has limited effect on small lesions, but is effective for large lesions or patients at high risk of postoperative bleeding (such as those receiving antithrombotic therapy).
ESD , the wound is removed and the exposed blood vessels are coagulated. Hemostatic clips can also be used to prevent clamping of large blood vessels.
Note:
For EMR of smaller lesions , routine preventive treatment is not recommended, but for large lesions or high-risk patients, postoperative preventive clipping has a certain effect (recommendation strength: Level 2, evidence level: C).
Perforation and bleeding are common complications of colorectal endoscopy.
Taking appropriate prevention and treatment measures for different situations can effectively reduce the incidence of sporadic diseases and improve patient safety.
We, Jiangxi Zhuoruihua Medical Instrument Co.,Ltd., is a manufacturer in China specializing in the endoscopic consumables, such as biopsy forceps, hemoclip, polyp snare, sclerotherapy needle, spray catheter, cytology brushes, guidewire, stone retrieval basket, nasal biliary drainage catheter,ureteral access sheath and ureteral access sheath with suction etc. which are widely used in EMR, ESD, ERCP. Our products are CE certified, and our plants are ISO certified. Our goods have been exported to Europe, North America, Middle East and part of Asia, and widely obtains the customer of the recognition and praise!

Post time: May-24-2025