

In the field of digestive disease diagnosis, endoscopy is one of the most essential tools. It includes gastroscopy, colonoscopy, enteroscopy, painless endoscopy, and others.
But what exactly are these procedures? Who are they suitable for? Who should avoid them? And what are the key preparation and post-procedure considerations?
Let’s explore each one.
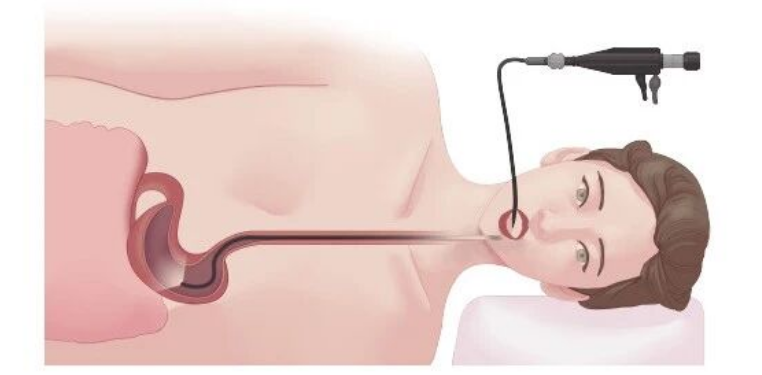
Gastroscopy
Gastroscopy allows direct visualization of the mucosa of the esophagus, stomach, duodenal bulb, and descending duodenum. It helps identify lesions, determine their nature, and obtain biopsy samples for histopathological diagnosis. It is commonly used to detect inflammation, ulcers, tumors, polyps, diverticula, strictures, malformations, or foreign bodies in the upper gastrointestinal (GI) tract.
Indications:
1.Upper GI symptoms (e.g., heartburn, dysphagia, epigastric pain, vomiting) with suspected esophageal, gastric, or duodenal disease requiring confirmation.
2.Follow-up or treatment evaluation of known upper GI conditions, such as peptic ulcers, esophageal cancer, or gastric cancer.
3.GI bleeding of unknown origin or location.
4.Suspicious upper GI lesions identified by imaging studies requiring characterization.
5.Presence of upper GI foreign bodies.
6.Need for endoscopic intervention, such as variceal ligation or sclerotherapy for esophageal varices, or endoscopic submucosal dissection (ESD) for early gastric cancer.
7.Family history of gastric cancer or other high-risk factors for gastric malignancy.
8.Confirmed H. pylori infection requiring assessment of gastric mucosal changes, or culture and antibiotic susceptibility testing to guide treatment.
Contraindications:
Absolute: Severe cardiopulmonary insufficiency, shock or critical illness, uncooperative patient, acute severe inflammation or visceral perforation along the insertion route.
Relative: Compromised cardiopulmonary function, bleeding tendency with hemoglobin 
Pre-Procedure Preparation:
1.Antiplatelet/Anticoagulant Agents: Patients on long-term aspirin, clopidogrel, warfarin, or similar medications should discuss discontinuation with their physician at least one week before the procedure to reduce the risk of major GI bleeding.
2.Fasting: No food or fluids after 10:00 PM the night before the examination.
3.Hypertension Medication: On the morning of the procedure, take antihypertensive medication with a small sip of water to prevent complications related to high blood pressure.
4.Diabetes Medication: Omit oral hypoglycemics or insulin on the morning of the examination.
5.Smoking: Patients should stop smoking at least one day prior to the procedure to reduce coughing during the examination. Smoking cessation also decreases gastric acid secretion, improving visibility.
6.Pre-Procedure Laboratory Tests: Complete blood count, liver function tests, coagulation profile, and infectious disease screening (e.g., hepatitis, HIV) are required.
7.Cardiopulmonary Evaluation for Elderly Patients: Chest X-ray, electrocardiogram (ECG), and echocardiography may be needed to assess tolerance to the procedure.
8.Post-Procedure Fasting: Due to residual pharyngeal anesthesia, do not eat or drink for 2 hours after the examination. After 2 hours, try a small sip of water. If no difficulty swallowing or coughing occurs, gradually progress to soft, warm foods.
9.Dietary Restriction: Avoid irritant foods for 1–2 days after the procedure.
10.When to Seek Medical Attention: Report severe abdominal pain or black, tarry stools to a healthcare provider promptly.
Risks and Complications:Complications such as bleeding, perforation, infection, arrhythmia, myocardial ischemia, pharyngeal injury, and temporomandibular joint dislocation are very rare during routine gastroscopy and can be minimized with adequate preparation and careful technique.
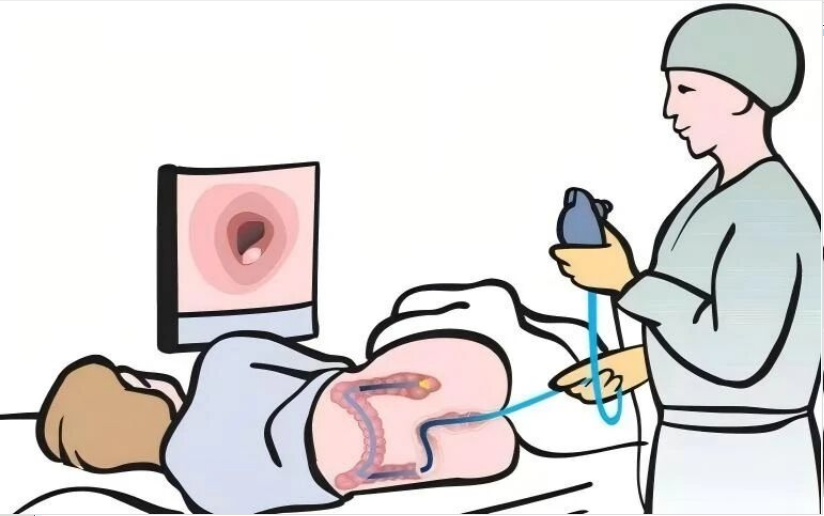
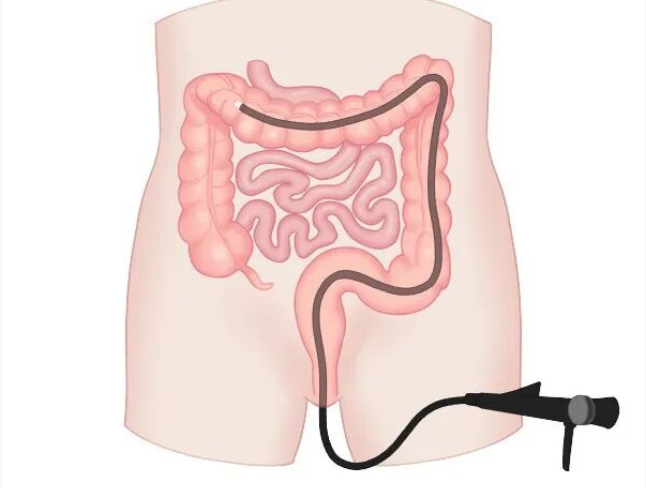
Colonoscopy
Colonoscopy enables visualization of the rectal, sigmoid, descending, transverse, ascending, and cecal mucosa, as well as the terminal ileum. It is primarily used to diagnose colonic and rectal inflammation, benign and malignant tumors, polyps, diverticula, and other conditions.
Indications:
1.Unexplained lower GI bleeding, including overt hematochezia or persistent fecal occult blood positivity.
2.Lower GI symptoms (e.g., abdominal pain, diarrhea, constipation, palpable mass, change in bowel habits) suggestive of colorectal disease.
3.Suspicious lesions detected by barium enema or imaging that require definitive characterization.
4.Differential diagnosis of inflammatory bowel disease (IBD), determination of disease extent and severity, and post-treatment follow-up.
5.Regular surveillance following colorectal tumor or polypectomy.
Contraindications:
In addition to those listed for gastroscopy, contraindications include intestinal obstruction, toxic megacolon, and allergy to components of the bowel preparation solution.
Pre-Procedure Preparation
Similar to gastroscopy, with the following distinctions:
1.Hypertension medication should be taken as usual on the morning of the procedure.
2.Diabetes medication should be omitted on the morning of the examination.
3.Low-residue diet (e.g., congee, noodles, bread, egg custard) the day before to improve bowel cleanliness.
4.No food after dinner the evening before (clear liquids allowed).
Bowel Preparation:
1.Adequate bowel preparation is essential to remove fecal material and allow clear visualization of the colonic mucosa.
2.Common cleansing agents in China include polyethylene glycol (PEG) electrolytes, 50% magnesium sulfate, and mannitol.
3.After taking the preparation, patients should walk around to stimulate peristalsis and accelerate elimination. Failure to do so may compromise bowel cleanliness.
4.If severe bloating or discomfort occurs, slow down or temporarily stop the solution, then resume once symptoms resolve. Clear, watery stools indicate adequate preparation.
5.For patients with inadequate bowel cleansing, a cleansing enema or repeated enhanced preparation may be necessary.
Post-Procedure Care:
1.Mild abdominal pain or bloating is normal and related to air insufflation during the procedure. No need for concern.
2.If severe pain, significant bloating, or rectal bleeding occurs, seek medical attention promptly.
3.Resume eating and drinking after symptoms subside. Start with soft foods (e.g., congee, fish) and avoid high-fiber or spicy foods.
4.Risks and complications (perforation, bleeding, infection, arrhythmia, myocardial ischemia, electrolyte disturbances) are rare and can be minimized with proper preparation and technique.
Endoscopic Ultrasound (EUS) – Ultrasound + Endoscopy
EUS combines endoscopy with high-frequency ultrasound. A miniature ultrasound probe is placed at the tip of the endoscope or passed through the working channel, allowing detailed examination of the gut wall layers and adjacent structures such as the liver, bile ducts, and pancreas.
While standard gastroscopy and colonoscopy are excellent for evaluating the mucosal surface, they cannot assess submucosal lesions or extraluminal structures. EUS fills this gap.
Indications:
1.Determine the origin and nature of submucosal tumors.
2.Assess depth of invasion of GI tumors and detect lymph node metastasis.
3.Evaluate resectability.
4.Diagnose benign and malignant lesions of the gallbladder and mid-to-distal common bile duct.
5.Evaluate pancreatic lesions.
6.Differentiate ampullary tumors.
7.Visualize mediastinal lesions.
8.Assess esophageal varices and response to sclerotherapy.
Contraindications:
1.Uncooperative patient
2.Suspected GI perforation
3.Acute diverticulitis
4.Fulminant colitis
5.Severe cardiopulmonary dysfunction
Painless Endoscopy (Sedated Gastroscopy/Colonoscopy) – Completely Comfortable
In painless endoscopy, the patient is positioned, a mouthpiece is placed, and oxygen is administered. A specially trained anesthesiologist injects a short-acting sedative (e.g., propofol) intravenously, inducing sleep within 30 seconds. The procedure is performed, and sedation is discontinued upon withdrawal. The patient awakens almost immediately.
Indications and Preparation:
Similar to standard gastroscopy and colonoscopy.
Contraindications:
1.Severe respiratory disease: Acute respiratory infection, pneumonia, severe COPD, acute asthma exacerbation, obstructive sleep apnea (OSA) with baseline hypoxemia.
2.Anatomic airway concerns: Limited mouth opening, restricted neck or jaw movement, or short, obese body habitus may compromise airway patency.
3.Poor general condition: Heart failure, myocardial infarction, stroke, coma, liver or kidney failure, severe anemia, myasthenia gravis, or frail, elderly patients.
4.High aspiration risk: Esophageal, cardia, pyloric, or intestinal obstruction, vomiting, or active hematemesis. Consider gastric decompression (nasogastric tube) prior to sedation.
5.Multiple drug allergies – allergic predisposition.
Pregnancy.
Pre- and Post-Procedure Considerations for Painless Endoscopy:
1.Avoid smoking the day before to reduce coughing during the procedure.
2.Have an adult family member or friend accompany you. Remove dentures before the procedure.
3.No food after dinner the night before. No clear liquids on the morning of the procedure.
4.Inform your physician of past medical history and drug allergies.
5.A companion should stay with you for 3 hours after the procedure.
6.Avoid spicy foods and alcohol for 8 hours after the procedure.
7.Do not drive, operate machinery, or work at heights for 8 hours after the procedure.
8.If an endoscopic intervention was performed, follow hospital observation or physician’s instructions.
Comfort (Transnasal / Ultrathin) Gastroscopy – Performed While Sitting and Talking
Comfort gastroscopy, also known as transnasal or ultrathin gastroscopy, causes minimal pharyngeal irritation and is nearly painless. Conventional gastroscopy uses an oral approach with a scope diameter of about 10 mm, often triggering significant gagging and nausea.
Transnasal gastroscopy uses an ultrathin scope with a diameter of only 5.9 mm. The procedure is comfortable, allowing the physician ample time for detailed examination and improving diagnostic yield.

Advantages of Ultrathin Gastroscopy:
1.Thinner: Conventional scope: 10 mm. Transnasal ultrathin: only 5.9 mm.
2.Less discomfort, fewer risks, fewer complications: Especially beneficial for children, critically ill, elderly, frail, and patients with compromised cardiopulmonary function.
3.Multiple insertion routes: Can be inserted via the nose or mouth without special handling.
4.Patient can talk during the procedure: Reduces anxiety and allows a relaxed, even pleasant, examination experience.
Indications and Contraindications:
Indications are similar to conventional gastroscopy. It is particularly suitable for patients with low tolerance for discomfort.
Contraindications: Nasal stenosis, significant nasal septal deviation, acute rhinitis. Although useful for some interventions (e.g., stent placement, jejunal feeding tube insertion), it is not suitable for polypectomy or hemostasis.
High-Definition (Precision) Gastroscopy / Colonoscopy – A Powerful Tool for Early GI Cancer Detection
Precision endoscopy is a recent concept aimed at improving the detection rate of early gastric cancer. It represents a major advance in early diagnosis, lesion assessment, and treatment guidance.
In practice, it combines high-definition white-light endoscopy with chromoendoscopy, electronic magnification, and targeted biopsy to minimize missed lesions.
When a suspicious lesion is identified or when a patient belongs to a high-risk group for gastric or esophageal cancer, precision endoscopy should be performed.

Key Differences from Standard Endoscopy
Personnel requirements: Must be performed by an endoscopist with specialized training in early cancer detection and extensive experience. A meticulous, “carpet” search of the esophageal, gastric, and duodenal mucosa is performed. Suspicious areas are further examined with chromoendoscopy, magnification, and precise biopsy to visualize microvascular and microsurface structures.
Equipment requirements: The endoscope must have high-definition magnification capability and electronic chromoendoscopy to enhance early cancer detection. When a suspicious lesion is found, chemical or electronic staining and magnification are used to define the location, extent, and morphology, with detailed documentation and photographic recording.
EUS may be needed for further evaluation.
Enteroscopy (Small Bowel Endoscopy)
Indications:
1.Unexplained diarrhea, abdominal pain, anemia, abdominal mass, nausea, or vomiting.
2.Unexplained GI bleeding or iron deficiency anemia.
3.Suspicious small bowel lesions on barium study or other imaging that cannot be characterized.
4.Follow-up of known small bowel diseases (e.g., IBD, polyposis, intestinal tuberculosis).
5.Family history of GI polyposis requiring small bowel examination.
6.Other systemic diseases or clinical findings necessitating small bowel evaluation.
Double-Balloon Enteroscopy (DBE)
Contraindications:
1.High risk of bleeding or perforation (e.g., GI perforation, severe enteritis)
2.Intestinal obstruction (contraindicates oral preparation and examination)
3.Severe cardiopulmonary, renal, or hepatic disease; uncontrolled hypertension; psychiatric illness
4.Other contraindications to upper endoscopy
Note: Due to technical difficulty and relatively higher risk, capsule endoscopy is now more commonly used for small bowel evaluation.
Capsule Endoscopy – Excellent for Gastric Cancer Screening and Small Bowel Disease
Capsule endoscopy involves swallowing a disposable, pill-sized capsule containing a camera and light source. As it travels through the GI tract via peristalsis, it captures images that are transmitted to a recorder worn by the patient. (Magnetically controlled capsule endoscopy, available in China, allows remote control of the capsule’s movement within the stomach.)
Indications:
1.Unexplained GI bleeding
2.Unexplained iron deficiency anemia
3.Suspected small bowel tumor
4.Suspected or refractory malabsorption syndrome
5.Detection of NSAID-induced small bowel mucosal injury
6.Clinically suspected small bowel disease
7.Monitoring and guiding treatment in Crohn’s disease
8.Surveillance of small bowel polyposis syndromes
Contraindications:
Absolute: No surgical capability or refusal to undergo abdominal surgery (if capsule retention requires surgical retrieval).
Relative:
1.Known or suspected GI obstruction, stricture, or fistula
2.Implanted cardiac pacemaker or other electronic device
3.Swallowing disorder
4.Pregnancy


Pre-Procedure Preparation:
1.Fasting: No food for 10–12 hours before capsule ingestion.
2.Bowel preparation: Same as for colonoscopy, performed the evening before to improve image quality.
3.Simethicone (optional): May be taken 30 minutes before the procedure to reduce bubbles.
4.Post-ingestion: Clear fluids allowed after 2 hours; light meal after 4 hours. The study ends when the capsule battery is depleted or the capsule enters the colon beyond the ileocecal valve.
Complications and Limitations:
1.Capsule retention: Defined as retention in the GI tract for >2 weeks. Requires surgical or balloon-assisted enteroscopic retrieval.
2.Aspiration into the airway is rare but possible.
3.Limitation: Capsule endoscopy cannot obtain tissue samples, limiting its ability to definitively diagnose certain lesions.
Behind every successful endoscopy procedure, reliable accessories play a critical but often overlooked role. From hemostasis to polypectomy and tissue sampling, the quality of consumables directly impacts clinical outcomes and workflow efficiency.
At ZRHmed, we focus on what passes through the scope:
Hemostatic clips for precise bleeding control
Polypectomy snares (cold and hot) for polyp removal
Sclerotherapy Needles for submucosal lifting
Cleaning brushes and other endoscopic accessories
With MDR CE certification and a growing global presence, we support endoscopy units and distributors with products designed for safety, reliability, and ease of use.
Because a great procedure needs not only a great scope – but also great accessories.
Conclusion
Gastrointestinal endoscopy remains the gold standard for diagnosing GI diseases. No advanced technology or device can replace it.
Do not be misled by claims such as “a single drop of blood for gastric cancer detection.” If you have GI symptoms, a proper endoscopic examination is essential.
Whether you need an endoscopy, which type is appropriate, and how to prepare should be determined by a specialist based on your individual condition. Proper preparation ensures patient safety and examination quality.
Wishing you long-term gastrointestinal health.
About ZRHmed
ZRHmed is a Chinese manufacturer of endoscopic accessories, including Biopsy Forceps, Hemostatic Clips, Polypectomy Snares, Sclerotherapy Needles, Spray Catheter, Cytology Brushes, Guidewire, Stone Retrieval Basket, Nasal Biliary Drainage Cathete etc. Our core products are MDR CE certified and used by distributors and healthcare providers worldwide.
We don’t make endoscopes. We make the tools that make them work.

Post time: Apr-28-2026